Online Learning Portal
Online Learning Portal

Hybrid Classes
We provide offline, online and recorded lectures in the same amount.

Personalised Mentoring
Every aspirant is unique and the mentoring is customised according to the strengths and weaknesses of the aspirant

Topicwise Mindmaps
In every Lecture. Director Sir will provide conceptual understanding with around 800 Mindmaps.

Quality Content
We provide you the best and Comprehensive content which comes directly or indirectly in UPSC Exam.

DAILY NEWS ANALYSIS
02 February, 2026
6 Min Read
India has committed to achieving Universal Health Coverage (UHC) through the National Health Policy (NHP), 2017 and Sustainable Development Goal-3 (SDG-3). The flagship programme driving this goal is Ayushman Bharat (AB). Despite notable progress, India still faces a significant access–affordability–quality gap, indicating that UHC objectives remain partially unmet.
What is Universal Health Coverage (UHC)?
Universal Health Coverage means that all individuals and communities have access to the full range of essential health services they need, without experiencing financial hardship.
Key Components of UHC
Access to Care: Everyone should be able to obtain necessary health services when they need them.
Quality of Services: Health services should be effective, safe, and of high quality.
Financial Protection: Individuals should not face financial difficulties due to medical expenses.
UHC is grounded in the universal human right to health, recognised in international covenants and reaffirmed by the Alma-Ata Declaration (1978), which prioritised comprehensive primary healthcare.
Need for UHC in the Indian Context
Historical Commitment to Universal Healthcare
The Bhore Committee (1943–46) recommended a tax-funded universal public healthcare system, rejecting an insurance-heavy model and emphasising preventive and primary care.
Policy Evolution After Independence
India’s National Health Policy, 1983 emphasised “Health for All”, highlighting the importance of primary healthcare and equitable distribution of resources.
Shift Towards Insurance-Led UHC
Schemes such as Rashtriya Swasthya Bima Yojana (RSBY), 2008 and Ayushman Bharat–PMJAY institutionalised UHC. However, these schemes reinforced a hospitalisation-centric, insurance-based approach.
Weak Public Health System and Rising Private Dependence
Chronic underfunding of primary healthcare has led to poor quality of public services and infrastructure gaps. National Sample Survey (NSS) data show growing dependence of the poor on private healthcare, leading to high out-of-pocket expenditure (OOPE) and rising household indebtedness.
Constitutional Basis for UHC
The Directive Principles of State Policy (Part IV) provide a constitutional foundation for the right to health:
Article 39(e): The state must secure workers’ health.
Article 42: Ensures just and humane working conditions and maternity relief.
Article 47: Directs the state to improve nutrition, living standards, and public health.
Furthermore, panchayats and municipalities are empowered under Article 243G to strengthen public health infrastructure.
Post-COVID Realisation
The COVID-19 pandemic exposed inequities in access to healthcare, highlighting the exclusion of informal workers and migrants and the fragility of hospital-centric, insurance-driven models.
Present Policy Direction
India currently aims to achieve UHC primarily through Ayushman Bharat–Pradhan Mantri Jan Arogya Yojana (AB-PMJAY), the flagship publicly financed health insurance (PFHI) scheme.
Challenges in Implementing UHC in India
Resource Constraints
India spends approximately 2.1% of GDP on public health, below the NHP target of 2.5%, which limits the ability to provide comprehensive services.
Infrastructure Gaps
Many rural areas lack adequate hospitals, clinics, diagnostic facilities, and medicines, which restricts access to care.
Healthcare Workforce Shortages
There is a shortage of trained medical personnel, particularly in rural areas, creating disparities in access and quality of care.
Fragmented Health System
India’s healthcare system is a mix of public and private providers, resulting in inconsistencies in quality, accessibility, and cost.
Federal Challenges
Health is a State subject, while financing and flagship schemes are centrally driven. This dual structure often leads to uneven outcomes across states.
Lessons from Global Experience
The Alma-Ata Declaration (1978) emphasised primary healthcare as the foundation of UHC.
Several East Asian countries initially adopted insurance-based UHC, but later strengthened primary and secondary care to manage ageing populations and chronic diseases.
Countries like China and South Korea achieved near-universal insurance coverage but faced high fiscal costs. China subsequently focused on:
Strengthening primary and secondary care
Emphasising prevention, early detection, and follow-up
Investing in human resources and population outreach
Maintaining a strong public sector to regulate private providers
Making Ayushman Bharat 2.0 More Effective
Shift from Coverage to Care
Move from hospitalisation-centric insurance to comprehensive, primary healthcare-led UHC, ensuring care is the first priority rather than insurance coverage.
Strengthen Primary and Secondary Care
Invest in health infrastructure, diagnostics, medicines, and referral systems
Use Health and Wellness Centres (HWCs) as gatekeepers to reduce avoidable hospitalisation
Increase Public Investment
Raise health spending to at least 2.5% of GDP and prioritise preventive and promotive care, including addressing social determinants of health.
Digital and Human Resource Reforms
Integrate ABHA IDs, interoperable health records, and disease surveillance systems
Address workforce shortages through task-shifting, local recruitment, and continuous training
Better Regulation and Strategic Purchasing
Implement standard treatment guidelines
Enforce cost controls and accountability mechanisms
Align insurance schemes within a robust public health system, ensuring efficiency and quality
Conclusion
While India has made significant strides toward UHC through Ayushman Bharat, persistent gaps in access, affordability, and quality indicate that a care-centred, publicly funded health system is essential. Strengthening primary healthcare, increasing public investment, integrating digital health tools, and regulating the private sector are key to achieving true Universal Health Coverage in India.
Source: THE HINDU

A year after tensions arising from Operation Sindoor, India and Azerbaijan have taken steps to restore and normalise bilateral relations. The 6th round of Foreign Office Consultations, held in Baku, marked the first such engagement since 2022, signaling renewed diplomatic momentum. Recent Diplomatic Engagement During the consultations, bo
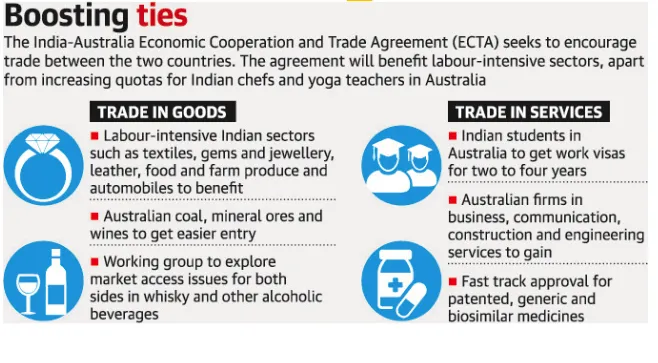
The India–Australia Economic Cooperation and Trade Agreement has completed four years since its signing. Both countries now aim to build on this progress through strengthened collaboration and ambitious targets, including reaching AUD 100 billion in bilateral trade by 2030. What is the India–Australia Economic Cooperation and Tra

A recent report by the Association for Democratic Reforms (ADR) analyses donations of ?20,000 or more declared to the Election Commission of India (ECI) by national political parties for FY 2024–25, highlighting transparency and accountability in political financing. Key Findings Massive Funding Surge Total donations to nationa
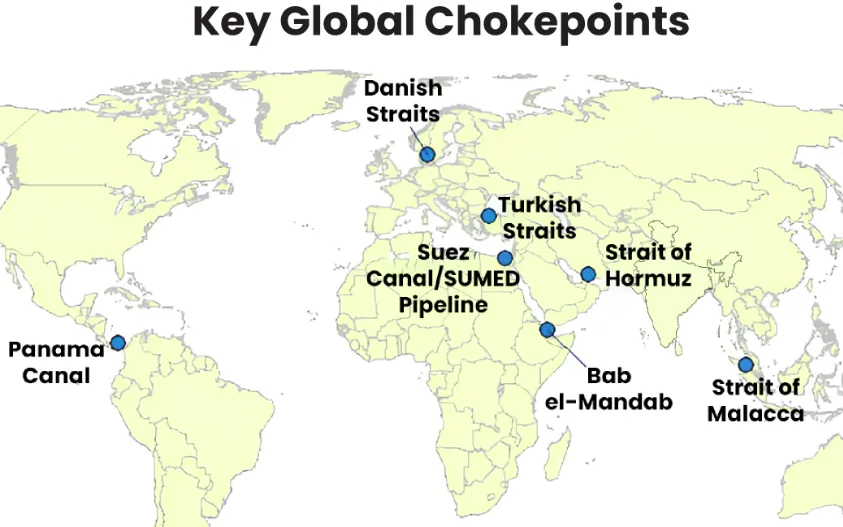
Maritime chokepoints are narrow channels along global shipping routes where maritime traffic is concentrated. These points are geopolitically and economically critical, as they handle a large proportion of global trade, especially energy shipments. Current Relevance Over two-thirds of seaborne energy trade passes through a handful o

Following the launch of Operation Epic Fury (U.S.) and Operation Roaring Lion (Israel), the geopolitical landscape has shifted fundamentally with the confirmed death of Iran’s Supreme Leader, Ayatollah Ali Khamenei.Iran retaliated through Operation True Promise 4, launching missile attacks against Israel and nearby Gulf states. The escala






Our Popular Courses
Module wise Prelims Batches
Mains Batches
Test Series
 My Notes
My Notes
 Geography And Environment
Geography And Environment


